




IMMUNOTHERAPY
Latest News

Latest Videos









CME Content





























More News

A team at Weill Cornell Medical College in New York that is studying ovarian cancer has not only discovered another mechanism by which tumors evade attack by the immune system, but is also devising a first-in-class potential treatment.

Study data reported at the 2015 ASCO Annual Meeting has demonstrated a nearly 20% response rate with the anti-programmed cell death-1 (PD-1) monoclonal antibody nivolumab (Opdivo) in patients with HCC.

An immunotherapy combination demonstrated an overall response rate of 27% in previously treated non–small cell lung cancer across a range of doses, according to results of an ongoing phase Ib study.

Patients with heavily pretreated colorectal cancer who harbored genetic defects in mismatch repair experienced high response rates when treated with the programmed cell death protein-1 inhibitor pembrolizumab (Keytruda), according to findings from an ongoing phase II study.

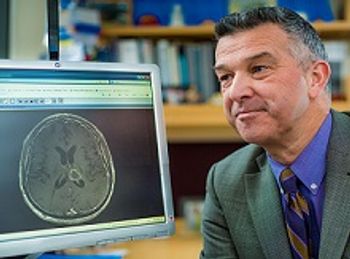
Targeted Oncology spoke with David Reardon, MD, clinical director, Center for Neuro-Oncology, Dana-Farber Cancer Institute, president of the Society for Neuro-Oncology, and lead author on the ReACT trial to better understand the significance of the study results for patients with glioblastoma.

Patients with pretreated advanced ovarian cancer demonstrated encouraging signs of antitumor activity with monoclonal antibodies against programmed death-1 and its ligand PD-L1, according to findings from two clinical studies presented at the 2015 ASCO Annual Meeting.

The FDA has granted a priority review to pembrolizumab as a potential treatment for patients with advanced non-small cell lung cancer following treatment with chemotherapy or a targeted therapy, if applicable.

Frontline nivolumab more than doubled progression-free survival (PFS), both as monotherapy and combined with ipilimumab compared with ipilimumab alone in patients with advanced melanoma, according to results from the phase III CheckMate-067 trial.

Nivolumab (Opdivo) improved overall survival and was less toxic compared with docetaxel in chemotherapy-pretreated patients with nonsquamous non–small cell lung cancer.

The anti-PD-1 antibody pembrolizumab produced broad and durable responses in patients with recurrent/metastatic head and neck squamous cell carcinoma.

MPDL3280A reduced the risk of death by 53% compared with docetaxel in previously treated patients with PD-L1-positive squamous and non-squamous non-small cell lung cancer.
Immune checkpoint inhibition will continue to attract interest at the 2015 ASCO Annual Meeting, with a number of abstracts focused on this emerging class of agents

Gary D. Steinberg, MD, Bruce and Beth White Family Professor, professor of surgery, director, urologic oncology, University of Chicago Medicine, discusses the impact immunotherapy has had on bladder cancer.

Treatment with the PD-1 inhibitor nivolumab demonstrated similar efficacy regardless of prior treatment with a BRAF inhibitor or ipilimumab in patients with BRAF mutant or wild type metastatic melanoma.

Optimal outcomes, and perhaps even a cure, could be achieved with the combination of targeted therapies and immune checkpoint inhibitors.
Two presentations at this yearâ��€™s American Association for Cancer Research (AACR) annual meeting linked a specific microRNA (miRNA), miR-34a, to an active area in immunotherapy, programed cell death-1 (PD-1) protein and its ligand, PD-L1.

Treatment with the PD-1 inhibitor nivolumab was active and tolerable across three doses for patients with metastatic renal cell carcinoma.

The PD-1 inhibitor nivolumab (Opdivo) has been has been assigned priority review designation from the US Food and Drug Administration (FDA) as a treatment for previously untreated patients with unresectable or metastatic melanoma.

MedImmune Limited, a subsidiary of AstraZeneca PLC, and Celgene International II Sà rl, a subsidiary of Celgene Corporation, have formed a strategic collaboration for the development and commercialization of AstraZeneca’s anti-programmed cell death-ligand 1 (PD-L1) agent MEDI4736.
Despite their promise, checkpoint inhibitors are not effective in every patient, and research suggests the STING (stimulator of interferon genes) pathway may hold important clues as to why some tumors fail to respond.

Mark R. Middleton, MD, PhD, discusses the results of a phase I/IIa trial of IMCgp100, a bispecific immunotherapy, for the treatment of patients with melanoma.

The PD-L1 inhibitor MPDL3280A demonstrated a 19% objective response rate (ORR) with 75% of responses ongoing in pretreated patients with metastatic triple-negative breast cancer (TNBC).
Results from the phase II, double-blind CheckMate-069 clinical trial showed unprecedented response rates with ipilimumab combined with nivolumab in previously treated patients with metastatic melanoma.

Jeffrey S. Weber, MD, PhD, a senior member at Moffitt Cancer Center, discusses toxicities associated with immunotherapies for the treatment of patients with melanoma.